Confocal laser microscope images tissue in vivo

Confocal laser microscope images tissue in vivo
Coherent illumination combines with scanning confocal techniques to yield a video-rate, micron-resolution
imaging system for noninvasive skin diagnostics.
Milind Rajadhyaksha and James M. Zavislan
Traditionally, biomedical imaging has been divided into capturing images of live tissue (in vivo) at relatively low resolution (from 10 to 1000 ?m) and capturing images of excised tissue at high resolution. In vivo imaging is usually performed using nonoptical modalities such as magnetic-resonance imaging, ultrasound, or x-ray tomography, which assess the general shape and appearance of tissue in its native state; however, this approach does not provide the cellular resolution necessary to analyze cell types and tissue morphology. To image tissue at high resolution using conventional optical or electron microscopes, one must slice the tissue into thin sections, otherwise the tissue above and below the layer of interest will produce out-of-focus reflections that seriously degrade image contrast.
Excising, fixing, and staining thin (and dead) tissue sections is time-consuming and expensive and produces image artifacts. For basic and clinical research a OwindowO into living tissue is needed. Biomedical researchers require an imaging technology that allows noninvasive cellular imaging of living tissue that is free from the artifacts of conventional microscopy and that also allows investigation of dynamic processes in tissue as a function of space and time. Applications include mechanisms of cell-cell interaction (diapedesis, phagocytosis, and pigment transfer), tissue regeneration and wound healing, microcirculation, delivery and distribution of drugs into tumors, physical and biological effects of light-tissue interactions, and characterization of diseases and cancers. Confocal microscopy offers one solution to this problem.
Confocal microscopes can noninvasively image tissue in vivo, with cellular-level resolution in organs such as the cornea and the skin.1-4 In human skin, confocal instruments have imaged the epidermis and dermis to depths of 300 ?m.5-9 Because confocal imaging inherently limits the imaging to a single section that is in focus, rejecting all the light that comes from out-of-focus sections, the approach permits high-contrast imaging of thick tissue sections.
In a confocal microscope, a point source of light illuminates a point inside the object (see Laser Focus World, Feb. 1994,
p. 83). The illuminated spot is then imaged onto a detector through pinhole, or Opoint,O aperture (see Fig. 1). This aperture acts as a spatial filter, rejecting light that is reflected from out-of-focus portions of the object to fall outside of the focal spot, so the resultant image has the high contrast of a thin-section image. To build an image using a confocal microscope, either the illumination spot or the object is raster-scanned mechanically or optically to swee¥an entire area.
Although in the configuration in
Fig. 1 light is transmitted through the object, in vivo imaging is based on the detection of reflected or backscattered light from the tissue; illumination and detection occur on the same side of the object (see Fig. 2). Signal contrast in confocal reflectance imaging appears to stem primarily from scattering resulting from the refractive-index variations of organelles and other structures.
In vivo confocal microscopy
Real-time, spot-scanning confocal microscopes for in vivo imaging have been developed in which the light collected by the detector maps the refractive index and absorption variations across the focal plane.10,11 The amount of light collected in each resolvable element of the image is a function of the incident irradiance, the scan velocity and imaging rate, the numerical aperture of the illumination and collection optics, the detector aperture size, the wavelength of illumination, and the scattering cross section of the tissue. For in vivo imaging, these parameters can be optimized to provide nearly diffraction-limited images of optically dense tissue such as skin to depths of 500 ?m.
Two of the most important performance parameters for confocal systems are the numerical aperture (NA) of the illumination and collection optics and the illumination wavelength (l). Assuming that the illumination and detection systems operate with equal numerical aperture in object space, the lateral resolution in the image for point objects is proportional (l/NA). Axial resolution, which defines the section thickness, is proportional to l/NA2.
For high-contrast imaging, the lateral and axial resolution must be limited to the lateral and axial dimensions of cells or other structures such as collagen (see Fig. 3). When we use a 100X objective lens with an NA of 1.2 and illumination at
1.06 ?m, the system achieves a lateral resolution of about
1 ?m and a sectional thickness of 4 ?m.
Our experiments with the Massachusetts General Hospital-developed confocal-scanning-laser-microscope research system for in vivo skin imaging have shown that for illumination wavelengths at 1.06 ?m, numerical apertures of 0.7 to 0.9 provide good image contrast down to a depth of 200 ?m. Imaging with numerical apertures higher than 0.9 should, in principle, improve resolution and contrast, but, in reality, suffers from increased off-axis aberrations, smaller fields of view, and reduced working distance. Imaging with numerical apertures lower than 0.7 provides poor contrast because the section thickness within the tissue exceeds the thickness of individual cell layers. With numerical apertures outside the optimum range, the sectioning and contrast degrade such that our confocal images look similar to those obtained with a conventional microscope.
A number of considerations drive the choice of illumination wavelength. Near-infrared radiation (0.7 to 1.2 ?m) penetrates dee¥into tissue because of decreased absorption and scattering, but also introduces disadvantages. At longer wavelengths, lateral and axial resolution decrease, increasing section thickness. The increased penetration by definition means reduction of the backscattered light that is detected to produce an image, which in turn reduces the signal-to-noise ratio.
When scanning object fields at video rates, we can detect 100 to 10,000 photons per pixel, depending on the depth of imaging. This light-starved condition forced us to choose an illumination wavelength that is well-matched to the peak sensitivity of easily available detectors. Silicon avalanche photodiodes offer sensitivity peaking around 800 nm and low-noise video-rate detection.
Wavelengths around 800 nm appear to offer a good compromise between increased penetration and good signal sensitivity for dermal tissue. However, one wavelength does not optimize the imaging of every tissue structure.
A further trade-off exists between the image frame rate versus detected signal level. To acquire high-fidelity images, the system required a frame rate high enough to reduce blur and motion artifacts in the tissue caused by either live-object motion or dynamic changes, such as blood flow in capillaries (see Fig. 4). For standard video scan rates and pixel densities, the pixel integration time is about 100 ns, and we detect only about one photon in one million. With this short integration time, quantum shot noise limits the signal-to-noise ratio and, thus, the maximum depth of imaging.
Because the detected signal is proportional to the incident power, increasing the irradiance at each pixel increases penetration depth. Incident power must be limited, however, to prevent optical damage to the tissue. The mechanism for tissue damage depends on the illumination wavelength. With wavelengths in the near-infrared, the tissue is damaged by heat from the absorbed radiation. Tissue exposed to 0.2 to
0.3 J/cm2 of energy at each pixel, at 800 to 1064 nm, has shown no damage when examined by histology. Higher energy densities may be possible to allow deeper imaging. This is an area of on-going research.
Prototype and clinical system development
Researchers at Massachusetts General Hospital (MGH) Wellman Laboratories developed and built a prototype confocal laser scanning microscope for video rate in vivo imaging (see photo on p. 119). It is designed to image the skin of patients for diagnostic purposes. A polygon and galvanometer mirror scan the illumination beam in two dimensions across an object located at the focus of the objective lens. A high-sensitivity avalanche photodiode detects the backscattered light, and a video monitor displays the image.
One important attribute of this system is its flexibilty: lasers with output wavelengths ranging from 488 to 1064 nm can be interchanged. By varying system parameters such as illumination wavelength, objective numerical aperture, and detector aperture, researchers are exploring the appearance of living cells inside tissue under different imaging conditions. Researchers are also compiling a database of in vivo confocal images of various lesions to compare with standard histological slides of the same lesions after removal. This work has shown that medically important features are visible, including cell shape and size, nucleus shape and size, nuclear-to-cytoplasm ratio, cell density, blood flow, distribution of melanin pigment, and the dermal-epidermal junction.
The MGH project demonstrates that near-infrared video-rate imaging provides a useful biomedical tool. In its present form, however, the microscope is not a simple-to-use biomedical imaging workstation. Lucid Technologies (Henrietta, NY) and MGH researchers are collaborating to develo¥a turnkey, user-friendly in vivo confocal system for general medical use (see table). The system retains the important attributes of the MGH system such as sub-second frame rates and low-noise detection, but is packaged in a tableto¥system slated for introduction in the first quarter of 1997. o
REFERENCES
1. T. Wilson, ed. Confocal Microscopy, Academic Press, San Diego, CA (1990).
2. M. L. Griem, A. Robotewskyj, and R. H. Nagel, Adv. Space Res. 14(10), 555 (1994).
3. B. R. Masters, ed., Selected Papers on Confocal Microscopy, SPIE Milestone Series Vol.
MS 131, SPIE Optical Engineering Press, Bellingham, WA (1996).
4. K. C. New et al., Scanning 13, 369 (l991).
5. J. B. Pawley, ed., Handbook of Biological Confocal Microscopy, 2nd ed., Plenum Press, New York, NY (1995).
6. P. Corcuff, and J. L. Leveque, Dermatology 186, 50 (1993).
7. P. Corcuff, C. Bertrand, and J. L. Leveque, Arch. Dermatol. Res. 285, 475 (l993).
8. C. Bertrand and P. Corcuff., Scanning 16, 150 (l994).
9. M. Rajadhyaksha et al., J. Investigative Dermatology 104, 946 (1995).
10. M. Petran et al., J. Opt. Soc. Amer. 58, 661 (1968).
11. R. H. Webb, G. W. Hughes, and F. C. Delori, Appl. Opt. 26, 1492 (1987).
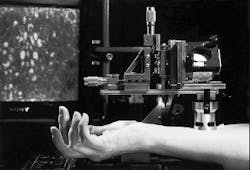
Scanning confocal microscope for in vivo, real-time diagnostics uses laser illumination to image skin tissue to depths of 500 ?m; monitor in background displays image.
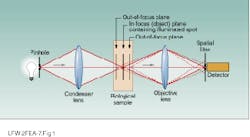
FIGURE 1. In confocal microscopy, a OpointO detector aperture spatially filters out-of-focus light reflected from tissue outside the plane of interest (dotted lines). Only light from the in-focus plane (solid lines) can be detected, allowing users to noninvasively image thin sections of transparent or translucent objects.
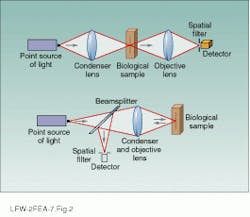
FIGURE 2. Confocal imaging can be done in two configurations:
transmission (top) or reflection (bottom). The reflected or backscattering approach is used to image living tissue.
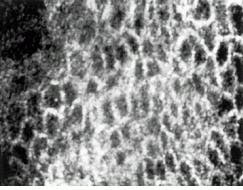
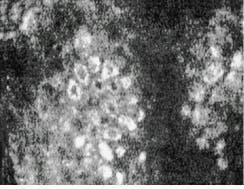
FIGURE 3. Laser-based confocal reflectance microscope produced these images of spinous cells in human skin at a depth of 50 ?m (top) and a cluster of basal cells in human skin at a depth of 100 ?m (bottom).
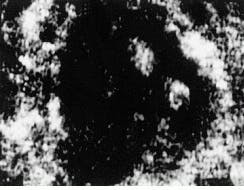
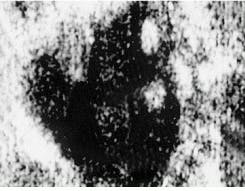
FIGURE 4. Time-sequenced confocal images show blood circulating in a human capillary at a depth of 200 ?m; bright disks are red blood cells