Flexible CO2 fiber tackles ‘inoperable’ conditions

MAX SHURGALIN, TAL DRORI, TAMIR WOLF, and VLADIMIR FUFLYIGIN
CO2 lasers have long been accepted as general surgical tools in dermatology, plastic and oral/maxillofacial surgery, otorhinolaryngology, gastroenterology, gynecology, and neurosurgery. Fundamental tissue-interaction properties and practical considerations have contributed to wide acceptance and perceived safety and predictability for precise tissue cutting, ablating, and simultaneous microvascular coagulation. Because the CO2 wavelength is strongly absorbed by water in biological tissues, penetration depth is on the order of 10 to15 µm, which means the CO2 beam can serve as an “optical scalpel” with precise control over tissue removal, and with minimal collateral thermal damage.1, 2 Concomitantly, the CO2 beam has some degree of functional hemostasis capacity, facilitating sealing of small- and medium-size blood vessels during soft tissue cutting and ablation.3 In addition to the continuous-wave (CW) mode of operation, CO2 lasers can be operated in a variety of pulsed modes delivering higher power in short time intervals, thereby increasing cutting and ablation speeds while minimizing damage to surrounding tissue.4, 5 Finally, CO2 lasers are fairly inexpensive, reliable, deliver high powers very efficiently, and require relatively little maintenance.
Realization of the full potential of CO2 laser radiation as a surgical tool in many disciplines, specifically those turning to minimally invasive approaches, has been limited by the absence of reliable flexible fiber-laser beam-delivery systems. Attempts to create a reliable fiber-optic system have resulted in developments such as solid-core fibers made of infrared transparent materials and hollow-core fibers using dielectric-metallic film mirror coatings.6 But none of these fibers provided the combination of safety, performance characteristics, reliability, and effectiveness necessary for surgical applications.
A different kind of hollow fiber
In 1998, a new kind of hollow fiber was invented at MIT: the hollow-core one-dimensional photonic-bandgap fiber.7 Instead of a dielectric-metallic mirror coating, a photonic bandgap implemented via an all-dielectric multilayer structure with high reflectivity for optical rays of all angles of incidence and polarizations (omnidirectional mirror) is used to confine and guide light though the fiber.8 The omnidirectional mirror structure, made of thin layers of two dielectric materials with alternating low and high refractive indices, is formed into a cylinder with the hollow fiber core in the center. The low-index material is a polymer and the high-index material is an infrared-transmitting chalcogenide glass. A thicker, all-polymer, cladding on the outside provides mechanical support for the mirror structure and gives desired mechanical properties.9 These photonic-bandgap fibers, made mostly of polymer with little glass consituent in the mirror structure, offer all the advantages of a hollow-core fiber combined with low optical losses, high mechanical flexibility, and robustness under bending, with bends as small as 2 cm in radius (see Fig. 1).
Despite very high reflectivity of the mirror structure, some of the guided radiation penetrates into the fiber walls, especially at locations in which the fiber is bent, and is absorbed by the polymer, which causes heating of the fiber. Even though overall heating is not significant, localized heating at bends limits the fiber’s power-handling capacity. Cooling gas can be flown through the hollow core of the fiber to alleviate the localized bend heating and increase power capacity and reliability. The gas also serves to purge the fiber core and clear the path of the laser beam, continuing on to clear the surgeon’s field of view from smoke and debris produced by laser interaction with target tissue.
Recently, significant improvements in materials, mirror design, and fiber fabrication technology resulted in development of flexible, mechanically robust, biocompatible, low-optical-loss fibers for CO2 lasers. These fibers afford reliability and power-handling capacity suitable for a variety of laser-surgery applications.10,11,12 A new polymer with relatively low absorption at the 10.6 µm wavelength is used in the latest generation of fibers, resulting in even lower transmission loss, especially at the fiber bends, thus enabling reduction of both the gas flow rate and fiber core diameter (for a given materials system, decreasing the core diameter increases fiber transmission loss and lowers fiber power capacity) without sacrificing power capacity or reliability. A new fiber-drawing process was developed for these fibers to match the different viscosity characteristics of the new materials system and to allow the fibers to be drawn into smaller inner and outer diameters. The advantages of smaller fiber OD and smaller fiber core include the ability to bend the fiber to smaller radii and a smaller output beam size (spot size) resulting in increased power density at the same power levels. These, in turn, result in a hightened cutting speed and augmented surgical precision.
The delivery system
The fiber system consists of three major components: a coupler for directing and coupling the laser beam into the fiber (a laser adapter), a beam-guiding fiber, and an application-specific distal tip with optional optics to shape the output beam. In addition, the system includes various procedure-specific handpieces with malleable straight and preshaped cannulas that assist the surgeon in manipulating the fiber and directing the output beam. Alternatively, the beam-guiding fiber can be introduced and manipulated via rigid and flexible endoscopes. The beam-guiding fiber and the distal tip are an integral device referred to as a BeamPath fiber. This fiber is a disposable, single-use device that is supplied sterile (gamma radiation at the dose of 25 to 40 kGy).
All BeamPath fibers custom connect to laser adapters that have been developed to fit the multitude of surgical CO2 lasers available in the market. The laser adapters are designed to provide efficient coupling of the laser beam into the fiber by optimal focusing of the beam into the core of the fiber. The laser beam is focused with an appropriate focal length laser-grade ZnSe lens with antireflection coatings, and is coupled into the fiber through the fiber’s ST connector (see Fig. 2). The adapter allows gas to be coupled into the core of the fiber as well; the gas is supplied to the main adapter body at a certain constant pressure and flows into the fiber core though the fiber connector with negligible gas leak at the connector junction. For sterile procedures the medical-grade gas is passed though a single-use sterile 0.2 µm filter before entering the adapter. A pressure regulator, manually set to correct pressure for each particular fiber product, controls the gas flow rate.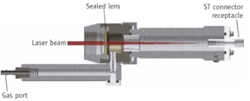
Designs for applications
The BeamPath fiber has an ST-type connector with a strain relief boot for easy and fast connection to the laser. The fiber is enclosed in a stainless steel braid-reinforced polyimide jacket, which provides additional mechanical support and protection from laser radiation in case of excessive fiber heating and failure. At the distal end, different tips are used, each designed for a specific medical procedure (see Fig. 3). The simplest tip design has a front opening in the jacket for the laser beam and forward gas flow and a number of side holes in the jacket that redirect the gas flow sideways, relieving gas pressure in case the tip comes in contact with tissue. The gas exiting the fiber coaxially with the laser beam also cools the tissue and keeps the target clean and free from debris and smoke, enhancing visibility and cutting precision. It may also aid in cauterization and coagulation by clearing the tissue from oozing blood and sealing the bleeding vessels underneath, an advantage compared to the line-of-sight laser systems.13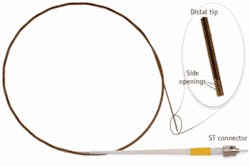

A number of fiber design modifications have been introduced to address specific requirements of different procedures.
Minimally invasive microsurgery
The OmniGuide BeamPath fiber was first used in a clinical setting in November 2004 to treat a patient suffering from recurrent respiratory papilloma of the airway that was unreceptive to prior treatment.12 For the first time, the surgeon was able to directly access and treat the lesions using the CO2 wavelength, which previously could not be applied due to lack of a flexible delivery system. Moreover, the patient, who could not tolerate general anesthesia, could be treated awake under local anesthesia.
Since this first case, the BeamPath fiber has been used in more than 7000 procedures. Introducing a paradigm shift in precision surgery, the fiber serves as a microsurgical instrument enabling access to a variety of anatomical locations. The unique tissue-interaction properties of the CO2 laser wavelength combined with indication-specific fiber designs and a range of small-profiled access tools allow surgeons to perform procedures in a minimally invasive fashion with increased precision.
In head and neck surgery, tools including micromanipulators and suspension laryngoscopes have been previously used to bring the CO2 laser beam to the target tissue. These techniques, however, necessitated an open surgical approach and were limited when trying to work around corners and in deep and difficult-to-reach regions. Today, head and neck surgeons are moving away from invasive treatment modalities such as radical neck dissection and radiation therapy to more minimally invasive surgical approaches. The ability to use the fiber as a precise scalpel in the depths of the glottis, supraglottis, oral and oropharyngeal cavities has enabled surgeons to perform more accurate resections in a less invasive manner.14 Based on preclinical data, the pin-point spot size of the flexible CO2 fiber enables precise cutting with minimal thermal damage to surrounding tissue. The importance of the latter is demonstrated, for example, in glossectomy procedures (resection of tongue cancer), where reduced thermal injury and charring allow pathologists to better assess tumor margins and delineate the border between cancerous and healthy tissue. Minimal thermal injury compared to the current standard of care (conventional electrocautery) may also be associated with less pain and a shorter time to first oral food intake.
Lasers have been widely accepted as no-touch, atraumatic tools in the treatment of hearing-related disorders. Hearing and balance, vital functions to everyday life, are controlled by the delicate organs and intricate anatomy of the middle and inner ear. Otologic surgery treats anatomy of submillimeter dimensions that is sensitive to mechanical manipulation and requires utmost precision. Flexible fiber delivery of CO2 laser energy to the confined and delicate middle-ear space provides a safe and precise alternative to other laser wavelengths in use.15 Otology fiber design with unique fiber-tip geometry and handpieces allows the surgeon to perform otologic procedures with ease and precision.
Brain tumors are among the most devastating conditions, and surgery often plays a pivotal role in treatment.16 Brain and spinal cord tumors are distinct from all other solid tumors in that resection is limited to the pathological tissue. In these cases, perhaps more than anywhere in the body, precision is of the essence. The use of lasers in neurosurgery was documented as early as 1966.17 However, previous laser systems were “bulky” to set up in the operating room, and provided less than optimal surgical control which marginalized lasers in neurosurgery. Current work done in this field indicates the value of the new fiber technology when operating near the delicate structures of the brain and spinal cord.
OmniGuide’s BeamPath fiber systems are continuously being tailor-fit to the needs of surgeons in various specialties. This precise, minimally invasive microdissection technology shows promise for a wide variety of additional surgical fields. Clinical studies are currently under way to establish evidence-based-medicine; our vision is that the flexible CO2 laser fiber will become a routinely used microsurgical instrument and part of every surgeon’s armamentarium.
REFERENCES
- T. Ohshiro, Lasers in Surgery and Medicine 6, p. 29 (1986).
- M. H. Niemz, Laser-Tissue Interactions: Fundamentals and Applic., 3rd ed. Berlin Heidelberg New York: Springer-Verlag (2003).
- G.P. Cram and M.L. Copeland, Phys. Res. B. 144, p. 256 (1998).
- M. Grimbergen CM. et al., SPIE 2975, p. 426 (1997).
- A.L. McKenzie, Physics in Medicine and Biology 35(9), p. 1175 (1990).
- J.A. Harrington, “Infrared Fiber Optics” in Handbook of Optics, New York: McGraw-Hill, V 4, ch. 14 (2001).
- Y. Fink et al., Science 282, p. 1679 (1998).
- B. Temelkuran et al., Nature 420, p. 650 (2002).
- G. Dellemann et al., Photonics Spectra 37(6), p. 60 (2003).
- C. Anastassiou et al., Proc.SPIE 5317, p. 29 (2004).
- Food and Drug Administration, Department of Health and Human Services, 510(k) clearance: K050541 Omniguide BeamPath CO2 Mark 1 Laser Beam Delivery System (2005), K070157 Omniguide BeamPath CO2 Mark III waveguide fiber (2007); K073313 Mark III waveguide fiber with low profile tip (2008).
- D. Torres et al., Proc. SPIE 5686, p. 310 (2005).
- A.K. Devaiah et al., The Laryngoscope 115, p. 1463 (2005).
- C.F. Holsinger et al., Int. J. Radiation Oncology Biol. Phys. 69: Supplement S129 (2007).
- G.S. Lesinski. “Lasers in Otology,” Glasscock-Shambaugh Surgery of the Ear, By A. Juliana Gulya and Michael E. Glasscock. Danbury: B.C. Decker Inc., p. 289 (2003).
- L.M. DeAngelis, N Engl J Med. 344, p. 114 (2001).
- H.L. Rosomoff and F. Carroll, Arch Neurol. 14, p. 143148 (1966).
Max Shurgalin is senior staff engineer, Tal Drori is product manager and biomedical engineer, Tamir Wolf is director of clinical affairs, and Vladimir Fuflyigin is director of R&D at Omniguide, Cambridge, MA, www.omni-guide.com. Contact Shurgalin at [email protected].